Materials and finishes - Internal Wall Finishes
CONTEXT
Overview – Finishes in the healthcare environment
Interior finishes play a vital role in a healthcare facility, as proper wall treatments can contribute to the creation and maintenance of a positive therapeutic environment for patients (Mayer , 2005)
Building finishes account for a large proportion of the overall cost of constructing a healthcare facility. According to Shohet et al. (2002), interior finishing and interior construction accounts for 32% of the initial budget. Maintenance and cleaning of finishes adds substantially to the ‘whole-life costs’ of finishes within a hospital or healthcare facility.
Despite this, finishes are often treated as optional and purely aesthetic components of the building and the spaces within it. When budget constraints are implemented, the finishes are usually the first area to suffer. Institutions will often standardise finishes across a spectrum of rooms/facilities for economy in replacement and/or cleaning regimes.
Interior finishes, however, play a vital role in the healthcare environment, and contribute substantially to the delivery of healthcare service and the protection of staff and patients.
“Until the germ theory was developed, more men were dying from small wounds and diseases than from major traumas on the frontlines. But as soon as germ theory was developed a whole new paradigm, a better way of understanding what was happening made dramatic significant medical improvement possible” (Covey, 1992)
In a study conducted by PricewaterhouseCoopers LLP (PwC) in association with the University of Sheffield and Queen Margaret University College, 2004, the comments from the majority of people who visited hospitals, including staff and patients, included “ cold, depressing, dehumanising, Kafkaesque, dirty, smelly, frightening, impersonal, confusing, dull shabby, windowless, grim, stressful…”. While it is a fact that most patients interviewed may have been negative as a result of their being ill, it does highlight a problem of the inhumane and threatening appearance of hospital environments (historically) where even more attention should be paid to creating a caring atmosphere.
 It is this paradigm shift that is required when considering and selecting finishes. The role of finishes in a healthcare facility has become as important an aspect of design as room sizes and relationships.
It is this paradigm shift that is required when considering and selecting finishes. The role of finishes in a healthcare facility has become as important an aspect of design as room sizes and relationships.
Building finishes are usually seen as a separate and final application to the building structure (Dean, 1996). There are however, instances where the finish is integral to the structure. These documents therefore include finishes and materials in such cases.
Suite of documents
This document forms part of a series of documents addressing internal materials and finishes in health facilities, which in turn forms part of the suite of documents created under the IUSS Project. The aim of the materials and finishes suite of documents is to provide guidance on design and specification for the various building components where current legislation, including the National Building Regulations, does not adequately cover suitability of finishes in the healthcare facility context.
While the guidelines speak mostly of new building work, most of the principles are consistent with refurbishment projects to existing buildings as well.
How to use this document:
Review the selection criteria – Part B
Select a room/department name in Part D, and note the performance category.
Refer to Table 1 for the properties that make up that performance category.
Refer to Part C to assess wall finish types that could satisfy those performance requirements.
Other IUSS health facility guides in this series include:
Internal Floor Finishes.
- Internal Ceiling Finishes
- Joinery and Storage Systems (to follow)
- Doors and Ironmongery (to follow)
- Sanitary Ware (to follow)
- Signage and Way-finding (to follow)
These guidelines are updated and revised periodically, and can be accessed at www.iussonline.co.za
The primary objective of this technical guide is to assist decision-makers with the selection of ‘appropriate’ wall finishes in the health facility context.
The guide looks at the context (Part A), then examines various selection criteria (Part B), then summarises technical information of various wall finishes (Part C) to assist with assessing the best finish for the facility. Finally, the selection criteria are grouped together to form performance categories (Part D) and a matrix of rooms, which indicates the most relevant performance category. The guide also examines various protection types to walls, including bump-rails and corner protection.
Policy context
This document offers guidance on the selection of appropriate wall finishes in health facilities. While the aim is to inform project and design teams about the wide range of considerations to take into account when selecting finishes, it does not diminish the responsibility of the design team to comply with all applicable professional and regulatory obligations and to specify materials and finishes ‘fit for purpose’.
Some of the pertinent regulations are the following:
SANS 204 Energy efficiency in buildings (general)
SANS 428 Fire performance classification of thermal insulated building envelope systems
SANS 1423-5 Performance requirements for textile fabrics of low flammability in movable office partitions
SANS 1449 Ceramic wall and floor tiles
SANS 2001 EC1 Construction works – ceilings and partitions
SANS 2001 EF1 Construction works EF1 – floor coverings and wall linings
SANS 2001 EM1 Construction works EM1 – cement plaster
SANS 2001 ET1 Construction works ET1 – tiling
SANS 4586 High and low pressure decorative laminates
SANS 10177 Fire testing of materials
SANS 10305 Paints, primers and varnishes – pigments, thickness, flexibility, impact and scratch resistance, washability, application
SANS 11890 Paints and Varnishes – determination of VOC content
SANS 13006 Ceramic tiles – definitions, classification, characteristics and marking
SANS 53163 Thermal insulation products for buildings (EPS)
SANS 53164 Thermal insulation products for buildings (XPS)
CKS 557 Wall coatings, resin solution base for interior and exterior use of plaster and concrete
CKS 564 Bonding liquid for porous surfaces
National Building Regulations and Building Standards Act, 1977 (Act 103 of 1977) amended 30 May 2008
- SANS 10400, Code of Practice for the application of the National Building Regulations, first rev. August 1990
- R158, Government Notice dated February 1980 (updated March 1993) Regulation pertaining to control of private hospitals, (revised 5 November 1996, but not gazetted).
- R187, Regulations governing private health establishments, Western Cape, 22 June 2001
The design principles on the above documents must be taken into account alongside the recommendations of this document. Furthermore, the South African National Standard (SANS) 10400 addresses numerous aspects involving materials and finishes. (Refer specifically to Parts J and T.) Current SANS applicable are as follows:
Other provincial policy documents are also applicable:
- KwaZulu-Natal, Department of Health Policy Document for the Design of Structural Installations, Rev.7, January 2013
- Eastern Cape Department of Roads and Public Works and Department of Health Hospital Design Guide, Rev. August 2004
SELECTION CRITERIA
Scope
The type and scope of activity in a space is one of the main factors that govern the selection of wall finishes in a healthcare facility.
(Onaran, 2009)
Healthcare facilities are complex buildings with spaces varying from general offices to highly specialised treatment areas. Each of these spaces has a specific need in terms of how the wall finishes should perform and how they can affect the perceptions and comfort of the user. Of the three dimensions of wall, floor and ceiling, the walls are most likely to be touched by the occupants, making them an important factor in terms of infection control. These and other criteria are discussed in more detail under selection criteria (Section C).
The healthcare environment is increasingly becoming a ’wheeled‘ environment, with everything from patients to equipment being moved on wheeled chairs, beds or trolleys of some kind. The wall finishes should be able to resist the accidental impact of trolleys and other objects. This is achieved by the inclusion of wall protection at strategic points. This guide examines the range of protection types available, and the advantages and disadvantages of their applications in the healthcare setting.
The following three basic categories of wall finishes should be considered:
- Liquid applied coverings
This includes paints such as PVA and enamel.
Flexible coverings
This includes vinyl cladding, linoleum, cork, carpet or wallpaper.
Hard, pre-formed finishes
This includes timber panels, ceramic and porcelain tiles, and the use of glass/glazed panels.
Each wall finish has different applications, resultant benefits and disadvantages. The various characteristics would need to be weighed against the functions of the various rooms within a healthcare facility.
Environmental aspects in the choice of finishes
A guide of finishes would be incomplete without highlighting the environmental aspects in the choice of finishes. This is an extremely broad factor that covers the following:
- Embodied energy of materials
- Life cycle costing and sustainability
- Toxicity and the effects of indoor environment quality
Embodied energy of materials
The term embodied energy refers to the total energy measure required to manufacture a product. This includes the following:
- Harvesting/mining of the raw material
- Processing the material
- Manufacturing the product
- Transporting/delivering the product to the manufacturing plant, retail outlets and finally the end-user
| Material | Embodied energy in MJ/kg (million joules per kilogram) |
|---|---|
| Concrete (in situ)
Hardwood timber, kiln dried, rough sawn Softwood timber, kiln dried, finished Cement Carpet (polypropylene/needle punch) Ceramic tile Vinyl sheeting Linoleum Solvent-based paint Water-based paint Wallpaper Gypsum plasterboard Medium-density fibreboard (MDF) |
1.0 – 1.6
2.0 2.5 7 – 8 95.4 2.5 79.1 116.0 98.1 88.5 36.4 6.1 11.9 |
Labour or mechanical energy spent on placing the product in its finished position
Buying locally produced materials is an easy and achievable way to lower the embodied energy of a building. The table below gives an indication of the embodied energy of various typical building materials.
Embodied energy of common wall finishes (and substrates)
Life cycle costs are described as the social, economic and environmental costs of a material or product from cradle to grave – that is, from the extraction of the raw ore needed to make it, through the manufacturing, to the end use to disposal or recycling (Daniel D. Chiras. The New Ecological Home, 2004).
While health facility design may limit your selection of materials in terms of other performance factors, which are more critical, every opportunity to reduce the embodied energy of materials should be pursued. Manufacturers increasingly aim at reducing embodied energy and the carbon footprint in the manufacture of their products. This is driven by the market demand and designers can contribute by choosing materials that support green initiatives in this regard.
Lifecycle costing and sustainability
The durability of materials is a key element in the life cycle cost assessment. A product may have a low embodied energy, but requires more frequent replacement in the building.
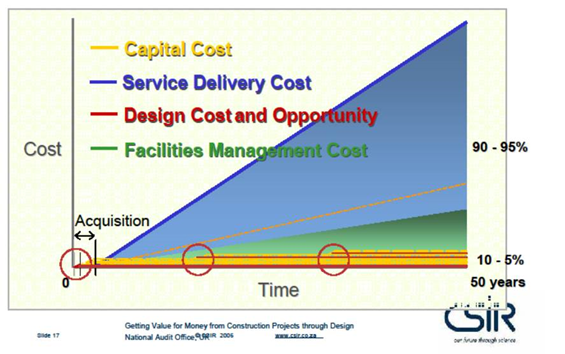
Specifiers should investigate the service life of materials with the respective manufacturers, to establish its lifespan. This element should also be highlighted to funders who often place more emphasis on reducing the capital cost of a facility, without considering the long-term cost.
The graph below indicates how capital outlay costs compare to lifespan costs – emphasising the importance of life cycle costs. Sustainability should be considered in all four stages of product life:
 Manufacture
Manufacture- Use
- Maintenance
- Disposal

The Green Building Council of South Africa has developed Green Star TM rating tools, which will credit materials with the following:
- Reuse of existing material
- Recycling properties
- Local sourcing
As a practical example, and to indicate the benefit of comparing life cycle costing, the table to the left shows the comparative life cycle costs of various floor finishes – in this instance demonstrating the low life cycle costs of a rubber product, even though the installation cost for this product was the highest at the outset.
Toxicity and effects on indoor environment quality
Indoor Environment Quality (IEQ) is one of the nine categories of the Green Building Council of South Africa’s Green Star TM Rating Tools. These rating tools are used to assess the environmental performance of a building and/or materials. By improving the IEQ, the wellbeing of the occupant is protected.
IEQ is measured in terms of the following:
- Internal noise levels (this is discussed in more detail under Selection Criteria: Acoustics)
- Mould prevention (this is discussed in more detail under Section Criteria: Humidity)
- Volatile organic compounds (VOCs)
Materials such as paints and polyvinyl-chlorides can emit VOCs (gasses) when finishes are new and then reduce over the lifespan of the product. Sealants and adhesives also give off VOCs, thus having a negative effect on indoor air quality.
VOCs can cause irritation and odour annoyance and could lead to behavioural, neurotoxic, hemotoxic and genotoxic effects (Meininghaus et al., 2000; Hoskins, 2003; Hodgson et al., 2000).
According to Hoskins (2003), VOCs can be carcinogenic, depending on the compound.
When considering the toxic impact on the environment in which the wall finish will be installed, the finish as a whole (complete with sealants, substrate material and adhesives) must be taken into account.
Another important aspect to consider is the use of non-toxic materials in mental health facilities, where patients are prone to chew and ingest any material that can be uplifted off surfaces, from paint to flooring.
Every effort must be made when specifying materials and finishes in these facilities to ensure that materials and their junctions are well secured and cannot be peeled back or picked off by patients. The toxicity of the material and/or content should be carefully considered to ensure it is appropriate for its location. The specifier should clarify the toxic content with manufacturers to ensure that these materials are safe and fit for this purpose.
Evidence-based design
Determining which criteria to apply when selecting finishes appropriate for health facilities could be very subjective. However, in recent years, there have been substantial advances made by various researchers in providing scientific evidence for the impact of the healthcare environment on healthcare outcomes. Many studies, such as Ulrich et al. (2008), demonstrated connections between the design of facilities and the effect on patients, staff and the public utilising healthcare buildings. This has led to a growing understanding of what the priorities in designing health facilities.
Extensive research by The Center for Health Design (CHD) Research Coalition on evidence-based Design led to the evidence-based design glossary, Phase 1 Report Healthcare Environmental Terms and Outcome Measures, November 2011.
Various unrelated research papers were gathered with interesting results. These included the following:
- Environmental factors influencing the contamination of inanimate surfaces, including interior finish materials of flooring and furniture, as well as surface cleaning methods (Anderson, Mackle, Stoler and Mallison, 1982; and Lankford, Collins, Youngberg, Rooney, Warren and Noskin, 2006).
- Reducing background noise in operating theatres and the impact on surgical errors (Moorthy, Munz, Dosis, Bann &and Darzi, 2003).
- Multiple environmental factors affecting patient fall rates (Calkins, Biddle and Biesan, 2011; and Becker et al., 2003).
- Patient satisfaction with quality of care when sound-reflecting ceiling tiles were replaced with sound-absorbing tiles to reduce noise (Hagerman and Colleagues, 2005).
- Positive visual distractions including windows, nature photographs, etc. and the effect on patients’ restless behaviour in waiting rooms (Nanda, 2010; and Pati and Nanda, 2011).
- Nurses’ exposure to daylight correlating to job satisfaction (Alimoglu and Donmez, 2005).
- Noise as a source of stress and its negative impact on staff (Morrison, Haas, Shaffner, Garett and Fackler, 2003).
“Ideal features of surfaces that satisfy sustainability, infection prevention and safe patient outcomes include cleanability, resistance to moisture and reducing the risk of fungal contamination.” (Bartley, 2010, based on CDC and HICPAC Guidelines, 2003)
Textile materials containing microbial agents (Takai et al., 2002).
- Aesthetic appeal and its effect on patient and staff satisfaction and patient waiting (Becker and Douglass, 2008).
An overview of these studies identified the following selection criteria:
- Infection prevention
- Cleaning and maintenance
- Safety
- Indoor air quality – humidity
- Indoor air quality – emissions
- Acoustics
- Aesthetics
Although all these factors are important, the specific functions of each space or room will re-order the priority of fulfilling each aspect.
To assist with establishing these priorities and assessing the effects of each criterion, these are examined in more detail in the next section.
Selection criteria
Infection prevention
The South African Patients’ Rights Charter (1997) states: “Everyone has the right to a healthy and safe environment that will ensure their physical and mental health or wellbeing including … protection from all forms of environmental danger, such as pollution, ecological degradation or infection.”
 According to a survey conducted by Rohde (2002), materials and finishes have in the past been selected according to the following characteristics in declining order of importance: aesthetics, durability, ease of maintenance, client preference, initial cost, cost of maintenance, infection control, ease of installation and life cycle cost.
According to a survey conducted by Rohde (2002), materials and finishes have in the past been selected according to the following characteristics in declining order of importance: aesthetics, durability, ease of maintenance, client preference, initial cost, cost of maintenance, infection control, ease of installation and life cycle cost.
Selecting the correct finish is a complex process with many aspects to consider, and the many and varied room types in a health facility extend the options. However, in healthcare facilities, the importance of the effect of a particular finish on the prevention of infection control must be prioritised. While it is understood that not every area of a hospital or health facility will carry infection prevention as the highest priority, this aspect remains the most pressing issue in the selection of finishes in health facilities.
The rising incidence of healthcare-associated infections (HAIs) in hospital and medical facilities supports the view that the selection of materials must first address infection prevention. This impacts on the choice of materials in two aspects. The first is whether the surfaces are likely to become reservoirs for infectious agents. This is a function of the surface conditions and structure of the finish. The second is the ability to clean the finish, which is discussed in the next section.
In order to keep wall finishes from transmitting harmful bacteria, they should be easy to clean and able to withstand repetitive wear and frequent germicidal decontamination, and have the ability to repel moisture
(Lankford et al., 2006).
The Center for Disease Control in the United States quoted statistics in 2010 of one out of every 20 hospitalised patients contracting HAIs, particularly in relation to sepsis and pneumonia.
| Risk categories | |||
|---|---|---|---|
| Extreme | High | Medium | Low |
| Operating theatres | General wards | Pathology units | Offices |
| Intensive care units | Dispensary production areas | Outpatients units | Engineering workshops |
| Sterile supply units | Treatment rooms | Dispensaries | Medical records |
| Neonatal | Nurseries | Radiology | Plant rooms |
| Delivery units | Kitchenettes/ward kitchens | ||
| Burn units | Mortuaries | ||
| Oncology units | Public areas | ||
| Renal units | |||
Although there is no known direct evidence linking HAIs in patients to particular finishes, there have been numerous studies conducted on microbial counts on floor finishes – particularly in soft textiles such as carpets. Beyer and Belsito (2000) proved that carpets acted as a reservoir for fungi and bacteria.
Lankford et al. (2006) examined different wall finishes after inoculation with Vancomycin-resistant Enterococci (VRE) and compared the results after seven days. The types of wall finishes tested included latex-based paint, enamel paint, vinyl, micro-perforated vinyl (with paper backing) and textured wallpaper. The report showed that all finishes still harboured some VRE pathogens that could be transferred through hand contact. The wallpaper and micro-perforated vinyl (used for printing large-scale wallpaper graphics) showed no reduction at all, indicating that the pathogens were harboured by these finishes. After cleaning and disinfection, results showed that latex paints did not clean as well as enamel paints.
The selection of finishes is still strongly linked to adequate cleaning and disinfection routines, and the location of the finish in terms of its performance. Notwithstanding, it is recommended that perforated finishes be avoided where patients are at greater risk of infection. Below is a table adapted from New South Wales Health: Infection Control Policy (PD 2007-035), which sets out patient risk categories:
“Outbreaks of infection have been related to the design, plan layout, function and/or finish of the built environment.”
(Cotterill et al., 1996 and Kumari et al., 1998)
When selecting finishes for a room/area that has an extreme or high infection control risk, special care has to be taken to select an appropriate finish. Nosocomial infections can be acquired in hospitals, nursing homes, rehabilitation centres and extended care facilities. Especially susceptible patients are immuno-compromised patients, the elderly and young children. These infections can be caused by unclean or non-sterile environmental surfaces.
Wall finishes that resist the spread of infection have qualities that can be summarised as follows:
- Smooth
- Impervious
- Joint-less/seamless
“Over the last few years, some carpet manufacturers have treated their products with fungicidal and/or bactericidal chemicals. Although these chemicals may help to reduce the overall numbers of bacteria or fungi present in carpet, their use does not preclude the routine care and maintenance of the carpeting.”
(Center for Disease Control –
Guideline for Environmental Infection Control, 2003)
On the opposite side of this spectrum, where infection prevention is the lowest priority, wall finishes have the following properties:
- Perforated
- Textured
- Jointed
 A note about anti-bacterial treatments and additives to wall finish products:
A note about anti-bacterial treatments and additives to wall finish products:
Some manufacturers tout the additional benefit of anti-microbial treatment in paints or grout to combat bacteria. The use of antimicrobial additives in the built environment is growing, for example - the impregnation of wood framing with silver nitrate to prevent microbial and mould growth, and extend the life span of the wood.
 Combined research by the US Environmental Protection Agency and the UK National Environmental Research Council is ongoing in this regard.
Combined research by the US Environmental Protection Agency and the UK National Environmental Research Council is ongoing in this regard.
A study by Noyce, Michels and Keevil (2006) compared the antimicrobial effectiveness of copper, brass and stainless steel. While the results indicated that copper had a better antimicrobial effect than stainless steel, the presence of dirt or dust may diminish that effect. The need for careful cleaning was highlighted.
The CDC HICPAC guidelines (CDC 2003) indicate that there is no evidence that antimicrobial-impregnated articles will prevent disease. There is a need for further research on products treated with these chemicals in terms of their potential risk and benefit.
Cleaning and maintenance
Cleaning and maintenance of walls is interconnected with infection control. The ‘washability’ of the wall finish will define the extent to which infectious agents can be removed and prevented from multiplying. For cleaning to be effective, the finish must be able to withstand regular and fairly vigorous cleaning.
Sufficient access to all areas of the finish or adversely the absence of any inaccessible gaps, voids and joints is of critical importance to prevent breeding areas for bacteria, etc.
A further aspect to consider is the level of disruption required to clean walls regularly. While textile finishes can reduce cold and institutional environments, they would be totally unsuitable in areas with a high infection control risk and a high incidence of soiling. It is also important for the paint or wall finish manufacturer to convey the cleaning and maintenance requirements to the end-user or institution for product guarantees to remain.. An effective cleaning regime is the primary means of defense in terms of controlling infection.
Wall finishes that are easily cleaned and have low dirt retention can be summarised as follows:
- Low maintenance
- Washable
Fire safety
The South African National Standard (SANS) 10400 lists specific requirements for hospitals and medical facilities with regard to the classification of internal finishes, irrespective of whether the area is sprinkler-protected or not. These materials are to achieve a Class 2 rating when tested in accordance with SANS 10177-3. The exceptions are the emergency routes where Class 1 is required.
- Internal finishes can be combustible but must comply with Class 2 (Part T – Table 9), except in emergency routes, where Class 1 is required.
- A dedicated section is written regarding operating theatres and intensive, high and critical care units and maternity delivery rooms , stipulating 120 minutes of fire resistance for division separations.
- A full list of materials deemed to be non-combustible is provided.
Note that these requirements are not room-specific, and are therefore considered a global requirement in the overall building, rather than for an individual space. The specifier would need to consult the fire regulations applicable to the building type and confirm that the products meet these requirements. The definitions in SANS 10400: Part A read as follows:
E2 Hospital: Occupancy where people are cared for or treated because of physical or mental disabilities and where they are generally bedridden.
E3 Other institutional (residential): Occupancy where groups of people who either are not fully fit, or who are restricted in their movements or their ability to make decisions, reside and are cared for.
E4 Healthcare: Occupancy which is a common place of long-term or transient living for a number of unrelated persons consisting of a single unit on its own site who, due to varying degrees of incapacity, are provided with personal care services or are undergoing medical treatment.
The requirements for finishes are set out in Part T of SANS 10400, and include the following:
Indoor air quality
There are two critical aspects to be considered when selecting wall finishes regarding indoor air quality. The first is the effect of the functions in that environment on the wall finish, namely water/moisture in wet spaces. The second is the effect of the finish itself on the air quality of the room in terms of the emission of VOCs.
Humidity
Certain rooms and areas of health facilities are wet spaces. These are spaces specifically used for the purpose of cleaning, washing, bathing or food preparation. These rooms generate more moisture than others, and as a result require moisture-resistant finishes. If the wall finishes are hygroscopic, these finishes can be prone to mildew and mould growth. Surfaces must remain dry and clean in order to prevent the growth of fungus (Hodgson et al., 2000).
Non-porous materials that do not absorb water are essential in these areas. These materials should also withstand regular cleaning, and should be able to withstand regular exposure to the moisture. Indoor air quality may be compromised by microbial contaminants such as mould, bacteria, allergens, chemicals, etc. in the air, which can affect the health of people. Where this is a requirement in wall finishes, this property is listed as:
High humidity
High humidity is considered as 25–100% relative humidity over an air temperature range of 10–30°C. A suitable finish should be able to withstand sustained contact with water vapour/water in these conditions. (Normal conditions would be considered as 25–65% relative humidity over air temperature range of 20–25 °C).
(National Health Services Health Technical Manual HTM56: Partitions)
Emissions from materials
As discussed under environmental aspects, the kind of wall finish installed can affect the environmental quality of the interior if VOCs are given off – commonly referred to as off-gassing.
These VOC emissions can be given off by:
- the product itself;
- the adhesives used to fix the product (for example, in the case of vinyl cladding or tiles);
- the sealants/grouts used to finish; and
- the cleaning solutions required for regular maintenance.
The smell of the interior of a new car – enjoyed by many – is an example of plasticisers that have evaporated (emissions that affect the indoor air quality). Various methods for measuring VOCs have been developed since the increase in awareness of these emissions and their influence on indoor air quality. The Green Building Council of South Africa awards points in the IEQ13 category where interior finishes minimise the contribution and levels of VOCs in buildings – with reference to paints, adhesives/sealants and carpets/flooring, where these products meet the indoor environmental quality (IEQ) levels as outlined.
Proper moisture control is essential in order to reduce health risks and sick building syndrome in an enclosed space (Mortenson et al., 2005).
The IEQ14 section measured the formaldehyde minimization, which is common with composite wood products. In addition, the MAT-7 section recognises the reduction of PVC products in the building materials used.
“Unnecessary noise is the most cruel abuse of care which can be inflicted on either the sick or the well.”
(Florence Nightingale, 1859)
It should be noted that primary VOCs decline quickly in the short term (less than one year), while secondary emissions can continue for the lifespan of the product, and should also be kept in mind when assessing this aspect of materials. Timing of the testing will yield very diverse results.
Patients with respiratory weaknesses such as asthma are most likely to be affected by VOC emissions. High-risk patients would benefit from materials that do not contribute to their condition. The ultimate goal of reducing emissions in the manufacture of building products should be to create a better and healthier environment for the patients and users of the facility.
However, the ‘order of magnitude’ should also be applied when using low VOC emissions as a criterion to select finishes. The use of vinyl sheeting, for example, may result in higher VOC emissions than, for example, ceramic tiles, but the infection control benefits of the seamless finish of the vinyl will outweigh the risks of VOC emissions. (More fatalities in patients have been linked to infection control issues than to VOC-emissions issues.)
The achievement of low VOC emissions should be a global criterion for a healthcare building rather than for one or more specific rooms, hence a separate criterion has not been listed for this item. More details on the VOC emissions of the individual wall finish types are provided in Section C.
“People who work in noisy environments for long shifts day in and day out, also have similar stress-induced experiences. They report everything from exhaustion to burnout, depression and irritability.”
S. Mazer –
Healing Healthcare Systems
Acoustics
Noise in health facilities is mainly generated by the following:
- Impact sounds, for example, pedestrian and wheeled equipment,
- bedrails moved up and down, doors closing and opening, footfalls, etc.
- Airborne sounds, for example, talking, medical equipment bleeps and alarms, nurse calls, PA system, etc.
Acoustical engineers at John Hopkins University found that the average (continuous level equivalent, LAeq) daytime hospital noise levels have risen from 57dBA in 1960 to 72dBA in 2006, with night-time sounds increasing from 42 dBA to 60 dBA over the same period. (HermanMiller Healthcare, 2006). An average motorcycle noise level measures 85 dB. The World Health Organization recommended an LAeq value of 30 dBA for ward areas.
Studies have shown that high levels of noise have negative physical and psychological effects on patients, disrupting sleep, increasing stress and raising blood pressure levels (Cmiel et al., 2004). The University of Michigan released a news brief in November 2005, showing that chronic noise increased the risk of heart-attacks in patients by 50% for men and 75% for women. The negative effect of chronic noise extends to staff as well. While the presence of electronic devices and healthcare apparatus, designed to give audible signals and alarms to the nursing staff of the patient’s vital signs, architects and health facility planners need to make an effort to minimise this effect of noise and alarm fatigue.
Long straight passages are perfect echo corridors, often amplifying noise levels. Disturbances in the sound path help limit the sound transmission by, for example, creating steps in the ceiling level or changing direction in the passageways.
According to Cmiel, et al. (2004), noise levels can reach those similar to jack-hammer levels at nurses’ stations during shift changes Consideration should be given to applying acoustic materials to these areas to maximise sound absorption where possible.
Recesses to accommodate noisy equipment can also be treated acoustically to reduce reverberation. Distance is also a good strategy (where feasible) as sound intensity decreases with distance, provided that the room dimensions and surfaces are designed so that there is very little reverberation.
Wall finishes that absorb sound, or at least do not contribute to noise levels, used in conjunction with sound-absorbent ceiling finishes should be used in key areas such as nurse restrooms or waiting areas where infection control requirements would not be as critical. In areas where sound reduction is rated as a high requirement (for example, ICU and general wards), this factor would be listed as “High acoustic”
Aesthetics
Research results from CABE, 2004 and 2005, King’s Fund, 2004, and Leather, Beale and Lee, 2000, all highlight the need for an integrated, holistic and sympathetic hospital aesthetic. Tofle et al. (2004) also emphasised the role of colour in healthcare environments. Key results show that the architectural setting, including finishes, has an effect on the patient’s experience, as well as the recruitment and retention of staff – a happy staff is more motivated to care for patients, who in turn recover more quickly. Paediatric wards particularly give an opportunity to set a playful scene and help young patients feel at ease. In public areas, more emphasis may be required for an attractive and welcoming interior.
Coloured and vinyl wallpaper can be used to good effect in passageways and public areas to set anxious patients at ease and create a cheerful atmosphere.
Colours and patterns can be used in wall finishes in health facilities for the following practical and aesthetical purposes:
 To improve the ‘institutional/cold’ interior look of the facility, room or area
To improve the ‘institutional/cold’ interior look of the facility, room or area- To be used for wayfinding, for example, colour-coding each department
- To create ’spaces’ by giving individuality to a specific area within a large open area

However, the following is to be considered:
- Excessive combination of colours and patterns is inappropriate in certain areas/rooms such as operating theatres.
- Some patterns and colours could impact negatively on certain patient groups, for example, the elderly or mentally ill.
- The wall finish must be adaptable should the space usage result in the need to change the aesthetics.
Where aesthetics is a primary requirement, this factor will be listed as:
- High aesthetics
TECHNICAL INFORMATION – WALL FINISH TYPES
“Wall finishes do change, due to changes in management or taste, and it is usually the first surface to be ’replaced’ or changed.”
(Vittori, 2002)
Liquid coverings
The quality of the wall finish (especially with liquid finishes such as paint), are only as good as the quality of the substrate. A poor quality plaster will not only affect the aesthetics, but also the integrity of the smooth impervious finish. Plaster cracks will be carried through almost all paints, and any crack can become a reservoir for bacteria. Bonding liquids could be used to some extent, but due to poor plaster sands and a lack of plastering skills, it is recommended that double plaster or skimming to finish a plastered wall be specified at the outset. (If the first plaster skin is approved, the second coat could be omitted.)
Paint (emulsion or oil-based)
- General description and properties
Paint is easily applied by a roller to a plastered wall surface. Following a primer and undercoat, three coats of paint are usually applied. Two-coat plaster is especially recommended where enamel paints are used, as any defects will be highlighted with these high-gloss type paints.
Figure 14
Paint types include emulsion paints which are water-based and produce a matt or silk effect – such as PVA. Oil-based paints like enamel dry to a hard, glossy finish that is impervious to water.
Paint is fairly inexpensive when compared to other wall finishes.
Infection prevention
The seamless finish produced by painted plaster makes this finish ideal for areas where infection prevention is paramount. There are no joints or crevices to encourage growth of microbes. Any mechanical damage can, however, lead to small cracks, and it is important to protect vulnerable areas. This is discussed in more detail under ‘Protection’. Studies have shown that PVA can be degraded by filamentous fungi, such as algae, yeasts, lichens and bacteria (Cappilelli and Sorlini, 2008). Paints with mould inhibitors and nano-technology enhancements are available on the market. Oil-based paints are more suited to areas that require high infection prevention criteria as the surface is impervious to water, oil and other fluids.
Cleaning and maintenance
The enamel and velvet sheen paints are highly washable, durable and stain-resistant. PVA can also be washed, but is not as stain-resistant or impervious and therefore not suitable in treatment areas. Paint is a low maintenance finish that requires re-application every few years (more often if mechanical damage occurs). Special attention should be given to the placement of switches and sockets in walls, as these areas are regularly touched, and can become infection-control risk areas if not kept clean. The smoother the surface, the easier it is to clean.
Fire safety
Paint is considered a non-combustible finish as the thickness of the paint is usually less than 0.5 mm. Refer to the manufacturer’s specifications and consult with SANS Part T to check the compliance and fire-resistance.
Indoor air quality: Humidity
Paints are generally not adversely affected by a reasonable amount of moisture being generated by the presence of taps or wet fittings in a room. Oil-based enamel paints are more resistant to moisture when compared to water-based PVA-type paints, and are therefore more suitable in wet or humid environments.
Indoor air quality: Emissions
The strong odour of a newly painted room is an indication of the high VOC emissions. Low-odour paints are marketed by manufacturers, and products with reduced or zero VOCs are being produced. Due to the increasing range of products and suppliers, the level of emissions should be checked with the manufacturer (refer to product-specific literature).
Acoustics
The hard surface of painted walls reflects sound and does not contribute to the impact of noise reduction or absorption. Where acoustics is a priority in a room or facility, other sound-absorbing products and finishes should be combined with the painted walls to achieve improved acoustics.
Aesthetics
 Paint is available in an extensive range of colours, and this is one of the great advantages of using paint. It provides a flexible means of adapting a space to suit the function of the room – from calming colours in a staff restroom, to cheerful and inviting colours in a doctor’s waiting room.
Paint is available in an extensive range of colours, and this is one of the great advantages of using paint. It provides a flexible means of adapting a space to suit the function of the room – from calming colours in a staff restroom, to cheerful and inviting colours in a doctor’s waiting room.
The effect of colour on healing has been well documented by Tofle et al. (2004).
Colour can also be used for the coding of areas – to demarcate different departments or floors of a multi-storey building. It can be effective in establishing zones for public and staff use. Paint can also be used to introduce colour for features or emphasis.
Private sector health facilities often make use of colour-branding for their facilities, and the use of specific combinations of colours becomes identifiable with the brand.
In public health facilities, the support of the Department of Health in the use of colour in this regard is paramount, as historically, decisions about colour have been based on ease of maintenance and whether new paints can match existing colours.
The colour codes and type of paints should always be included in the as-built documents to assist managers to obtain the correct paint.
Epoxy coatings
General description and properties
There are two main types of epoxy coatings – water-borne and solvent-borne coatings. Both types have improved properties compared to water- or oil-based paints, including the following:
- Chemical and abrasion resistance
- Outstanding adhesion to a variety of substrates
- Excellent toughness, hardness and flexibility
- Superior dimensional stability
- Heat resistance
Water-dispersed epoxy coatings are resin-based wall coatings of between 0.3 and 0.5 mm thick. A primer or pore-filler coat is first applied to smooth plaster, followed by two coats of epoxy wall coating applied with a roller. This creates an impermeable seal on the wall surface with a gloss finish.
The use of water in lieu of solvent in the coating means less hazardous material for the environment, and reduced odours/fumes.
Solvent-borne epoxy paints are more economical, but should not be exposed to extensive sunlight as this leads to chalking and degradation. The solvent-based epoxy coating is also toxic when wet, unlike the water-borne version, but once dry, the solvent-borne epoxy coating is also non-toxic. Special precautions need to be taken when applying this product. Primers are also required, and solvent-based epoxy coatings can be applied with a roller, brush or airless spray.
Infection prevention
The water-borne epoxy resin coatings have been tested under ISO 14644, which classifies different materials according to their cleanliness in terms of the particle and airborne molecular contaminants that are emitted or released by the finished product. This is critical in industrial environments where optical or electronic goods are manufactured, or where food is processed. Water-dispersed epoxy resin wall coatings are one such product that satisfies the criteria and is approved for use in ‘cleanroom’ settings.
Cleaning and maintenance
The impermeable finish is smooth and non-porous, making it easy to clean, highly washable, durable and stain resistant. Colour variation in different batches of solvent-based epoxy coatings is expected.
Fire safety
Since the epoxy finish is less than 0.5 mm, it is considered a non-combustible finish (once dry). Refer to the manufacturer’s specifications, and consult with SANS Part T to check compliance and fire-resistance.
Indoor air quality: Humidity
Epoxy coatings have good water-resistance and are suitable for use in moist/humid areas as the finish is hydro-phobic and prevents the ingress of moisture.
Indoor air quality: Emissions
Solvent-borne epoxy coatings produce a strong odour in a newly painted room, unlike water-dispersed epoxy coatings. The development of water-dispersed epoxy coatings has been hastened by the move away from VOC emissions in paints to meet air quality standards.
Acoustics
The hard surface of epoxy-painted walls reflects sound and does not contribute to the impact of noise reduction or absorption. Where acoustics is a priority in a room or facility, other sound-absorbing products and finishes should be combined with the painted walls to achieve improved acoustics.
Aesthetics
Epoxy coatings are available in a muted range of pastel colours. Although the colour range and variety is more limited than regular paints, the comparative expense of epoxy coatings usually means it is used for its superior performance properties, and less likely for its aesthetics.
Flexible sheeting
Vinyl wall cladding

Vinyl wall cladding, as in the case of vinyl floor sheeting, is manufactured from a combination of vinyl resin and various additives, such as the following:
- Plasticisers – used to make the sheet more flexible.
- Stabilisers – to minimise degradation and discoloration.
- Pigments – for colours and patterns
- Fillers – such as lime or other locally available material
Vinyl cladding is generally 1.25 mm thick, but sheeting that is 2 mm in thickness can also be used. Depending on the manufacturer, it is supplied in 1.2 m- or 2 m-wide rolls. Vinyl cladding is sometimes used as a dado cladding in passageways or high-traffic areas due to its durable, resilient and impervious finish.
Vinyl cladding can be supplied with a specialised polyurethane-resistant (PUR) surface treatment. This coating improves resistance to staining and cleaning chemicals and supports indentation recovery.
Infection prevention
Vinyl sheeting, as a material, has been found to inhibit the growth of bacteria, and particularly Methicillin-resistant Staphylococcus aureus (MRSAs). The welded joints prevent dust or dirt from congregating in areas that are difficult to clean, and the integral skirting supports this seamless appeal. This has made vinyl sheeting very suitable for use in healthcare facilities. However, the adhesives behind the cladding are important for the success of this wall finish from an infection-prevention aspect, as any lifting away from the wall or failure in the application of the adhesive will create voids in which bacteria or insects can breed. If the wall is mechanically damaged in any way, even the finest of cracks will provide the access needed to these voids. Ends should be well sealed and any area at risk of being damaged should be protected. Refer to the section on bump-rails and protection.
Cleaning and maintenance
The cladding is easily washed, which contributes to its performance as a hygienic wall finish. Vinyl cladding is not easily damaged, and when treated with a polymer dressing/surface treatment, is low-maintenance. When maintained properly, the sheets have a long lifespan, and are therefore fairly cost-effective in comparison to other wall finishes. Cladding with PUR treatment requires only spray-and-dry buffing for general cleaning, although water-based dressings are beneficial. Special cleaning solutions are used for heavy staining, but abrasive cleaning methods should not be used. If portions of the wall cladding are damaged, replacement of a section is difficult as the stripping off of adhesives may require re-plastering prior to applying the new cladding.
This is also very disruptive in high-use areas. Colour matching is also difficult when replacing panels as colour batches will vary.
This is, however, a low-maintenance, flexible covering that is not likely to crack with small movements in the wall.
Cleaning should always be carried out in accordance with the manufacturer’s specifications to comply with material warranties. The specifier should ensure that these instructions are included in handover packs issued to the building owner/user when occupation takes place.
Fire safety
In terms of SANS 10400, operating theatres, ICUs, high-care or critical care units, and maternity delivery units are required to have walls with a fire-resistance of 120 minutes. The effect of the finish, in conjunction with the wall structure, should be checked with the manufacturer for compliance in this regard.
Indoor air quality – Humidity
Vinyl sheeting is well suited to areas of high humidity, and wet areas such as sluice rooms.
Indoor air quality – Emissions
Some manufacturers have addressed VOC emissions in their products and indicate a pass in VOC emissions tests as well as Building Research Establishment (BRE) A+ ratings. Materials are 100% recyclable or contain a percentage of recycled materials. Each supplier will differ, and the specifier should check these aspects when considering a product. VOC emissions of adhesives and sealants, where applicable, are also to be considered.
Aesthetics
 Vinyl wall cladding is available in subtle pastel colours that can contribute to creating a calming/soothing effect. The application of cladding requires skill to apply and if the substrate plaster is not completely smooth below the surface, the vinyl cladding will amplify imperfections and could look unsightly.
Vinyl wall cladding is available in subtle pastel colours that can contribute to creating a calming/soothing effect. The application of cladding requires skill to apply and if the substrate plaster is not completely smooth below the surface, the vinyl cladding will amplify imperfections and could look unsightly.
Acoustics
Vinyl sheeting is softer than tiled surfaces, with better sound absorption qualities than hard finishes.
Wallpaper murals
General description and properties
Digitally printed wallpapers are becoming more popular in public areas of health facilities. These murals can be custom-sized and printed to any image and can make a strong contribution to introduce outdoor and nature scenes where external windows and natural light is not possible. The murals are supplied in panels that generally overlap and are glued to a substrate that should be smooth, sound and dry. A lining paper can be applied prior to the finish paper. Wallpapers generally have a textured matt finish, which can be cleaned. Self-adhesive papers which are PVC-free are also manufactured. The wallpaper generally has a latex-saturated paper backing.
Infection prevention
While some wallpapers can be cleaned, micro-perforated vinyl, which is commonly used for large-scale digital prints, were found to perform poorly when inoculated with pathogens. These wallpaper murals should not be used in areas where patients are immuno-compromised, especially if the prints can be touched easily. The joints between the panels – although sealed with the glue used to affix the mural, mean that the surface is not seamless. By applying a clear varnish sealing coat over the product, the infection prevention is improved.
Cleaning and maintenance
Light cleaning with a soft, non-abrasive cloth – which can be damp – will allow for regular cleaning, but the wallpapers are susceptible to stains. Any mechanical damage to the mural will be difficult to repair. The location of these murals should be carefully considered, as the images will lose their effect if bump-rails run clear across the image. If well cared for, though, the murals require little maintenance.
Fire safety
Self-adhesive wallpapers have been tested in accordance with EN13501-1:2007 and were classified as B-s1, d0 (fire behaviour (B), smoke production (Class 1), flaming droplets(0)). In terms of SANS 10400, operating theatres, ICUs, high-care or critical care units and maternity delivery units are required to have walls with a fire-resistance of 120 minutes. The effect of the finish, in conjunction with the wall structure, should be checked with the manufacturer for compliance in this regard.
Indoor air quality: Humidity
The paper constituents of this product and the micro-perforations make it unsuitable for use in high-humidity areas.
Indoor air quality: Emissions
The adhesives used to install the wallpaper are often high in VOC emissions, although PVC-free self-adhesive papers are produced. In comparison to paints, however, the emissions are lower.
Acoustics
Wallpaper is softer than tiled surfaces, with better sound-absorption qualities than hard finishes. Thicker and heavily textured papers will aid sound absorption.
 Aesthetics
Aesthetics

The aspect of aesthetics is where wallpaper scores well. The use of high-resolution photographic images in murals can contribute almost as much as a real view of a natural environment. This is useful where external windows are not feasible. This can also be used to good effect in staff restroom areas, cafeterias or foyers.
Hard preformed coverings
Porcelain or ceramic tiles
General description and properties
Porcelain and ceramic tiles generally provide a durable, aesthetically acceptable wall finish that is moisture-resistant. A wide spectrum of tiles is available in varying sizes, material composition, quality and cost, resulting in varying performance. Porcelain and/or ceramic tiles are most commonly used in health facilities in wet areas, such as bathrooms, kitchens, and utility and cleaning areas due to the impervious quality and performance under wet conditions. The use of unglazed tiles is not recommended in health facilities as these absorb moisture and other fluids, which may be present in kitchens, mortuaries, etc.
The specifier should research the actual tile carefully, ascertain if the product is imported, what long-term stocks would be available, and ensure the tiles have been sufficiently cured. Where possible, the specifier should use full-bodied porcelain tiles rather than glazed porcelain or ceramic tiles. This is evident in the following comparison between the general properties of the two tile types:
Full-bodied porcelain tile:
- Colour is throughout, as the term ’full-bodied‘ implies.
- Squareness of tiles is consistent with minor deviations.
- Tile sizes are consistent with minor deviations.
- Smaller joints can be used, due to tile size consistency.
- Flatness of tile face is consistent.
Glazed ceramic tile:
- Colour is a glaze on top of the tile that can wear or chip off.
- Tile sizes can vary.
- Squareness of tiles can vary.
- Wider joints are required, due to size and squareness inconsistencies.
- Tiles are often not flat and edged surfaces tend to dip, resulting in rough surfaces.
Infection prevention
Although an individual tile unit complies with selection criteria such as being impervious and easy to clean, a finished tiled wall, including grout and movement joints, provides a less favourable result in terms of the following:
- Grout in the joints is porous and can retain moisture, which encourages the growth of mould.
- Grout joints pose a potential infection-control risk in small cracks and openings that form between the tile edge and the body of the grout.
- Tiles may crack and chip when trolleys bump against them, creating small cracks where moisture can be retained and microbes can grow.
- Replacement of these damaged tiles or re-grouting is disruptive to the daily operations of the facility, and matching existing tiles can be difficult.
Anti-fungal grout will contribute to the control of mildew, but cannot replace good maintenance regimes.
Cleaning and maintenance
Porcelain wall tiles generally need to be cleaned with water and a cleaning agent. For oily spatter in hospital kitchens or body fluids or chemicals in laboratories or mortuaries, appropriate cleaning is required. The ease of cleaning, as well as the durability of the tiles under rigorous cleaning regimes, makes a tiled wall suitable in areas where splash-back is common – such as above sinks and hand basins.
Fire safety
Porcelain is non-combustible in terms of SANS 10400: Part T. In terms of SANS 10400, operating theatres, ICUs, high-care or critical care units and maternity delivery units are required to have walls with a fire resistance of 120 minutes. The effect of the finish, in conjunction with the wall structure, should be checked with the manufacturer for compliance in this regard.
Indoor air quality: Humidity
The polished or glazed surfaces of the tiles make them highly suitable and unaffected by high humidity in the room. However, as mentioned above, the joints are susceptible to moisture-retention and encourage mould and microbe growth in the minute cracks and gaps. Proper scrubbing and regular maintenance will inhibit fungal contamination. The use of epoxy grout is recommended (and not cementitious grout). Epoxy grouts are resin-based, and repel moisture, which inhibits the growth of mould.
Indoor air quality: Emissions
Porcelain tiles and cementitious grout (not recommended in health facilities) do not generate VOC emissions, but some adhesives, other grouts, sealants and cleaning agents generate VOC, which affect the indoor air quality. The production of tiles has a high-energy input, with high sustainability production costs and production emissions.
Acoustics
 Tiled walls are hard surfaces that do not absorb any sound and will contribute substantially to noise in the healthcare setting. This is due to the reflective surfaces on walls, causing echoes. Where the function of the room does not warrant special attention to acoustics, and other criteria have priority, then tiled walls are suitable.
Tiled walls are hard surfaces that do not absorb any sound and will contribute substantially to noise in the healthcare setting. This is due to the reflective surfaces on walls, causing echoes. Where the function of the room does not warrant special attention to acoustics, and other criteria have priority, then tiled walls are suitable.
Aesthetics
Tiles are available in a wide selection of colours, shapes and sizes. This allows for visually appealing, non-institutional aesthetics in health facilities. Since the surfaces do not scratch or scuff easily, the aesthetic appeal is durable. A variety of stainless steel or PVC tile-in trims are available to finish the edges of tiles on walls or reveals. These also provide some protection to the exposed edge.
Timber panelling
General description and properties
Timber panelling creates a warm, welcoming environment and can be used in certain areas of healthcare facilities.
The most common locally available timber is meranti and pine, which is available in various standards and quality. The versatility of the timber products provides almost unlimited options in terms of cladding walls or creating features from wood, ranging from standard tongue-and-groove planks to slatted battens and perforated acoustic panels. The timber is usually varnished or painted for internal use. Engineered timber products are also available with melamine and veneer finishes.
Infection prevention
Timber is a source of nutrients to bacteria, and good maintenance and cleaning will be needed to ensure that mould and other bacteria are prevented from establishing. Timber would not be suitable for areas where a seamless finish is required due to the jointing. Acrylic resin-based anti-bacterial varnish may extend the lifespan of the timber.
Cleaning and maintenance
The timber panelling is usually finished with varnish or sealant that is water-resistant and therefore washable, but access to narrow grooves may limit the effectiveness of cleaning. Occasional re-varnishing would be required, which could be disruptive to the activities in such areas. Engineered medium-density fibreboard (MDF) wall panels do not require repainting if clad, but should not come into contact with water.
Fire safety
Timber is combustible, and in terms of SANS 10400: Part T, internal finishes can be combustible, but must comply with Class 2 (Part T: Table 9), except in emergency routes, where Class 1 is required. Specific requirements are listed for operating theatres, ICUs, high-care or critical care units and maternity delivery units in that these areas are required to have walls with a fire resistance of 120 minutes. The extent and effect of the timber finish, in conjunction with the wall structure, should be checked for compliance in this regard.
Indoor air quality: Humidity
Well-varnished timber will be protected from the effects of moisture, but generally timber should not be used in rooms where humid and moist conditions persist. MDF wall panels are not suitable for humid or wet areas.
Indoor air quality: Emissions
 Timber is a natural product that does not emit VOCs, but the finishing specification, such as varnish, is often a source of VOCs. Engineered timber products, such as MDF board, contains a higher resin-to-wood ratio than any other urea-formaldehyde pressed wood product, and is recognised as being the highest formaldehyde-emitting pressed wood product. (US Environmental Protection Agency). These VOCs are fairly quickly dissipated. Refer to product-specific literature.
Timber is a natural product that does not emit VOCs, but the finishing specification, such as varnish, is often a source of VOCs. Engineered timber products, such as MDF board, contains a higher resin-to-wood ratio than any other urea-formaldehyde pressed wood product, and is recognised as being the highest formaldehyde-emitting pressed wood product. (US Environmental Protection Agency). These VOCs are fairly quickly dissipated. Refer to product-specific literature.
Aesthetics
The warmth of wood grains, with their natural beauty and range of timber hues, is a sought-after aesthetic that is being replicated in many other finishes, such as ceramic tiles, vinyl and wallpaper. Original wood finishes are unique without production pattern repetition. This is the appeal of timber.
Acoustics
Slatted or perforated timber panels are well suited to rooms that require acoustic performance, such as conference rooms, prayer rooms or quiet spaces. Perforated surfaces aid in reducing the retransmission of sound and can assist where many other surfaces are hard and reflective.
Glazed partitions
General description and properties
 There are areas in the healthcare environment that can benefit from the use of glazed partitions to improve the visual supervision of the occupants – for example, in isolation or paediatric wards. All glass in healthcare facilities must have safety glazing, but some additional protection should be included at critical heights where bump-rails would normally be fixed. This can be done using the aluminium frames and mullions at the correct heights.
There are areas in the healthcare environment that can benefit from the use of glazed partitions to improve the visual supervision of the occupants – for example, in isolation or paediatric wards. All glass in healthcare facilities must have safety glazing, but some additional protection should be included at critical heights where bump-rails would normally be fixed. This can be done using the aluminium frames and mullions at the correct heights.
Provision must be made for blinds or curtains to allow for privacy or room darkening when needed. Glass also brings the opportunity to allow natural light into deep spaces where external windows cannot be accommodated. Alimoglu and Donmex (2005) reported that nurses’ daily exposure to daylight correlated positively with job satisfaction. Berry and Parish (2008) reported that nursing staff who worked in a new unit that featured (among other aspects) more natural light, were more satisfied and less stressed. Stress negatively reflects on staff job satisfaction, which in turn correlates with staff turnover.
 Exposure to daylight reduces depression among patients, decreases length of stay, improves sleep and circadian rhythms, lessens agitation among dementia patients, and eases pain (Joseph 1999).
Exposure to daylight reduces depression among patients, decreases length of stay, improves sleep and circadian rhythms, lessens agitation among dementia patients, and eases pain (Joseph 1999).
Infection prevention
Glass is impervious and unaffected by moisture or water, and is easy to clean, making this a useful wall finish in high-infection control areas. The key is in how the joints are treated. Welds on frames should be continuous – leaving no gaps or small apertures for moisture or bacteria to gain access. Gaskets in the aluminium frames must seal the junctions with glazed panels to support proper cleaning. Blinds should be encapsulated in double glazing to maintain the hygienic finish.
Micro-perforated vinyl stickers can retain moisture and harbour pathogens, and special attention to cleaning procedures for these areas should be highlighted.
Cleaning and maintenance
Glass walls require occasional washing, but the glass is waterproof and unaffected by most cleaning agents and acids. Glass can also be supplied with proprietary films that ’self-clean‘ by using sunlight and rain to wash off organic dirt. These are suitable for external glazing only.
Fire safety
Both glass and aluminium (cast or extruded) are categorised as non-combustible materials in terms of SANS 10177-5. Internal finishes can be combustible, but must comply with Class 2 (Part T: Table 9), except in emergency routes, where Class 1 is required. Specific requirements are listed for operating theatres, ICUs, high-care or critical care units and maternity delivery units in that these areas are required to have walls with a fire resistance of 120 minutes.
Indoor air quality: Humidity
Glazed walls are well suited to humid environments as they are unaffected by moisture.
Indoor air quality: Emissions
 While the production of glass may emit VOCs, glass is inert and impermeable and does not emit VOCs. Coatings to the framework may, however, emit low VOCs. Refer to product-specific literature.
While the production of glass may emit VOCs, glass is inert and impermeable and does not emit VOCs. Coatings to the framework may, however, emit low VOCs. Refer to product-specific literature.
Aesthetics
In a well-maintained facility, glass walls can give a clean, open feel to the healthcare environment. The aesthetics can be improved by what lies beyond the glazing – especially if there is a view to be admired. An open configuration provides the caregiver or visitor with a more ‘global’ view of the unit, and allows immediate assessment of the status. This transparent aesthetic can improve order and cleanliness standards in the facility.
Acoustics
Glass is a hard, reflective surface that will not absorb sound, but possibly add to noise scatter.
Bump-rails
 Beds, food trolleys, medicine trolleys, drip stands, mop buckets and wheelchairs are just some of the types of wheeled equipment common in the hospital or healthcare environment. This often leads to accidents and mechanical damage to walls, corners and exposed edges. Bump-rails should be specified and fitted in key areas to minimise repairs and prolong the wall finishes. In addition, bump-rails are useful behind chair-backs in waiting areas, where scuff marks are common.
Beds, food trolleys, medicine trolleys, drip stands, mop buckets and wheelchairs are just some of the types of wheeled equipment common in the hospital or healthcare environment. This often leads to accidents and mechanical damage to walls, corners and exposed edges. Bump-rails should be specified and fitted in key areas to minimise repairs and prolong the wall finishes. In addition, bump-rails are useful behind chair-backs in waiting areas, where scuff marks are common.
Most damage to walls will be prevented by running a bump-rail at around 900 mm above the floor (to the centreline), with a depth of 200 –300 mm. The areas behind beds or cots can be deeper at around 600 mm. Some trolleys also have projections at low level, and the equipment to be used in the particular area should be considered when setting heights and spacing of bump-rails.
Some bump-rails simply consist of sheeting of only a few millimetres thick, cladding the wall at a particular height, but the offset type of rail that projects away from the wall is more effective in protecting the surface, as the force of the impact is difficult to predict or contain. These projecting rails have the added benefit of providing a hand-hold for patients who are walking in the passage.
The different types of commonly used bump-rails are summarised below.
Laminated or solid timber bump-rails
General description and properties
 Timber bump-rails are relatively inexpensive and easy to manufacture and fit. These can be routed, and shaped into solid timber sections, or smooth laminated timber sections. The benefit of using timber is that sections that may become damaged are easy to replace. The use of timber creates a warm, welcoming environment. The most common locally available timber is meranti and pine, which is available in various standards and quality. The timber is usually varnished for internal use.
Timber bump-rails are relatively inexpensive and easy to manufacture and fit. These can be routed, and shaped into solid timber sections, or smooth laminated timber sections. The benefit of using timber is that sections that may become damaged are easy to replace. The use of timber creates a warm, welcoming environment. The most common locally available timber is meranti and pine, which is available in various standards and quality. The timber is usually varnished for internal use.
Infection prevention
Timber is a source of nutrients to bacteria, and good maintenance and cleaning will be needed to ensure that mould and other bacteria are prevented from establishing. Timber would not be suitable for areas where a seamless finish is required due to jointing, small ledges and recessed areas. Acrylic resin-based anti-bacterial varnish may extend the lifespan of the timber.
Cleaning and maintenance
The timber panelling is usually finished with varnish or sealant, which is water-resistant, and therefore washable, but access to narrow grooves may limit the effectiveness of cleaning. Occasional re-varnishing would be required, which could be disruptive to the activities in such areas.
Aesthetics
The warmth of wood grains with their natural beauty and range of timber hues is a sought-after aesthetic, which is being replicated in many other finishes, such as ceramic tiles, vinyl and wallpaper. Original wood finishes are unique without production pattern repetition. This is the appeal of timber.
Extruded PVC bump-rails
General description and properties
Pre-formed rigid PVC bump-rails are fitted over aluminium retainers with rubber inserts, which help absorb any impact. The PVC covering is scratch-resistant with a textured surface. These rails can either be flush-mounted against the wall with an overall thickness of about 20–35 mm, or mounted on aluminium brackets at regular centres, usually less than one metre apart, and standing 50–100 mm proud of the wall surface. Continuous timber backing rails can also be fitted where anti-ligature options are needed in mental health facilities.
The bump-rail size can vary between 50–200 mm in height. Injection- moulded plastic joiners and end-caps are available in matching colours.
Hollow, rigid extruded PVC bump-rails are also available, with PVC brackets, but these should only be used with solid timber inserts as the unsupported PVC has been known to become brittle over time. Flexible PVC hand-rail covers are also manufactured to fit over steel brackets, with a width of 50 mm.
Infection prevention
 Vinyl/PVC provides no nutrient source for bacteria in which to thrive, and regular cleaning will ensure a hygienic product. Special attention should be paid to cleaning hand-rails as these have more angles and recesses and are more likely to be touched.
Vinyl/PVC provides no nutrient source for bacteria in which to thrive, and regular cleaning will ensure a hygienic product. Special attention should be paid to cleaning hand-rails as these have more angles and recesses and are more likely to be touched.
Cleaning and maintenance
The manufacturer’s instructions must be followed for cleaning procedures and products to prolong the lifespan of the bump-rails. If a section becomes damaged, the relevant section can be replaced, although colour may vary slightly.
Aesthetics
The PVC bump-rails are available in a wide range of colours to complement the interior colour scheme. Bump-rails also provide an opportunity to introduce bolder colours, and can be used as markers to follow or define different departments.
Tubular stainless steel bump-rails
General description and properties
Stainless steel bump-rails are sturdy, hard-wearing, easy to clean and an elegant solution for wall protection. Tubular bump-rails for internal areas should be manufactured from Grade 304 stainless steel, and are usually 32 mm in diameter. A wall thickness of 2 mm is recommended to withstand impact. External rails in coastal regions should be made from Grade 316 stainless steel. Material test certificates should be requested from the supplier to indicate the manufacturer, grade, chemical and mechanical specifications. All joints should be specified as fully seam-welded, including where stanchions are fixed to the rail and fixing plates. The screws/bolts and nuts used for fixing the flanges must be the same grade as the tubular rail. Flanges should be a minimum of 6 mm thick. All welded joints should be cleaned of residue prior to pickling and passivation. The tungsten inert gas (TIG) process of welding should be specified as this produces a better-quality weld on a wider range of thicknesses of stainless steel sheeting.
Best corrosion-resistance will be achieved by pickling all fabricated items using commercially available products. The item is then thoroughly rinsed with water to remove all traces of acid and is then passivated with nitric acid passivating solution, and rinsed again.
Infection prevention
Stainless steel provides no nutrient source for bacteria in which to survive, but dirt build-up on the surface can become a source of bacteria. Although copper has better anti-microbial properties than stainless steel (Noyce, Michels & Keevil, 2006), stainless steel is a more durable and cost-effective solution and performs better than most other materials in terms of preventing the transmission of pathogens.
Cleaning and maintenance
Stainless steel is a very low-maintenance product that has longevity superior to most other products available. However, like any surface, the build-up of dirt and dust will affect the performance and lifespan of the product and regular cleaning is required. Stainless steel should be cleaned with a soft cloth, regular household dishwashing liquid and warm water. In coastal areas, stainless steel finishes should be cleaned every four weeks, and every 4–6 months in inland areas. Without regular cleaning, the protective chromium-oxide film will be contaminated by dirt build-up on the surface, thus trapping these corrosive agents.
 Aesthetics
Aesthetics

Stainless steel creates an impression of cleanliness, with its smooth, shiny surface. The seamless rails also add to the hygienic appeal. This bump-rail solution has been used widely in hospital environments.
Cladding to medium density fibreboard substrate
There are various cladding options when using MDF board as a substrate for bump-rails. The surface finish products can be moulded around the MDF substrate, and the shape and size is only limited by the ability of the cladding to follow the radii of corners and edges.
Suitable adhesives would need to be considered and should be checked with the respective manufacturers of the cladding product selected. The rear of the bump-rail should be fitted with melamine or similar covering to prevent moisture ingress and balance the board.
These bump-rails can be fitted flush against the wall, or fixed with a purpose-made bracket or timber spacer behind them.
Engineered timber products, such as MDF board, contain a higher resin-to-wood ratio than any other urea-formaldehyde pressed wood product, and is recognised as being the highest formaldehyde- emitting pressed wood product (US Environmental Protection Agency). These VOCs are fairly quickly dissipated.
The cladding options commonly used for bump-rails include the following:
Vinyl sheeting
The advantage of using vinyl on a bump-rail is that the joints can be welded for a seamless finish. This is beneficial in terms of infection control. Mechanical damage can cause fine cracks that would be difficult to repair without replacing a section. The vinyl finish can also match the floor sheeting if required.
Refer to sections on vinyl flooring or wall cladding for general descriptions and performance of vinyl.
Solid surfacing
These smooth resin-based finishes are heated and moulded to the substrate, allowing for seamless curves and corners. Small cracks due to mechanical damage on solid-surfacing can be easily repaired by sanding and re-sealing. These cracks could present an infection-control risk, as these fine apertures can be difficult to see, and moisture can penetrate to the substrate below and become a reservoir for bacteria.
The solid-surfacing is available in a wide range of colours from vibrant flat colours to stone-speckled patterns and translucent pigmented options. Since this product can be used on joinery and counters, the bump-rails can be made from matching or complementary colours.
Carpeting
Carpet cladding on bump-rails will contribute to sound absorption, but is not recommended in clinical areas as bacteria can be retained in the fibres, and these textile finishes are difficult to keep clean. Refer to sections on carpeting for general descriptions and performance of carpets.
Stainless steel cladding
 Stainless steel sheeting can be bent or curved to follow simple profiles, and can be glued with appropriate adhesive, as well as mechanically fixed with screws. Edges should be sealed with silicone. The stainless steel cladding should not be less than 1.5–1.6 mm thick on bump-rails to be able to withstand impact. Standard finishes include brushed satin (matt) or a bright annealed (shiny) polished finish. A brushed satin finish will be less likely to show fingerprints, while a shiny finish will easily reveal fingerprints. Both finishes should be cleaned with a soft cloth, warm water and regular household dishwashing liquid at least once every four weeks.
Stainless steel sheeting can be bent or curved to follow simple profiles, and can be glued with appropriate adhesive, as well as mechanically fixed with screws. Edges should be sealed with silicone. The stainless steel cladding should not be less than 1.5–1.6 mm thick on bump-rails to be able to withstand impact. Standard finishes include brushed satin (matt) or a bright annealed (shiny) polished finish. A brushed satin finish will be less likely to show fingerprints, while a shiny finish will easily reveal fingerprints. Both finishes should be cleaned with a soft cloth, warm water and regular household dishwashing liquid at least once every four weeks.
Refer to the section above on stainless steel tubular bump-rails for general descriptions and performance of stainless steel.
Corner protection
Protection is needed on external corners and exposed edges of walls in healthcare facilities, as these areas are generally subject to more impact than walls in straight runs. The detail must be considered in conjunction with the bump-rail, as the two items will meet at the corner. The bump-rail can be continuous in the horizontal line, with the corner protection only covering the wall below. Alternately, the corner protection can be continuous in the vertical line, and the bump-rail can stop short of the corner on each side. A projecting bump-rail will still afford some protection to the corner, over and above the corner protector plate.
Corner protectors should cover at least 1 m from the floor, but where taller food trolleys or laundry trolleys are used, the full height of the wall may need to be protected.
 Stainless steel corner protectors
Stainless steel corner protectors

Stainless steel corner protectors are fitted to exposed corners using stainless steel screws and adhesive, and are usually 50 x 50 mm in size, depending on the detail of the bump-rail at the corner. The corner edges should be rounded as they can be very sharp.
A thickness of 1.5–1.6 mm is recommended to give best impact protection. Refer to the section above on tubular steel bump-rails for general properties, performance, cleaning and other recommendations for the specification of stainless steel. Grade 304 is recommended for internal areas. Screws used for fixings must be the same grade as the angle.
Columns are also high-impact areas in open spaces, and stainless steel sheeting provides a neat solution where rigid aluminium, timber or MDF substrates cannot be fitted to such tight curves.
 Vinyl corner protectors
Vinyl corner protectors

Proprietary systems of vinyl corner protection are available on the market in rigid extruded high-impact resistant PVC. Some systems can be supplied with aluminium retainers where higher impact is expected.
These PVC corner protectors have a fine textured scratch-resistant finish, and are available in 50 x 50 mm or 70 x 70 mm sizing and are 1.2 mm thick. Standard heights are 1.2 m high.
 They are fixed using approved adhesives, but screws can also be used. A range of colours is available to match the PVC bump-rails.
They are fixed using approved adhesives, but screws can also be used. A range of colours is available to match the PVC bump-rails.
PERFORMANCE
Performance categories
The properties described in the selection criteria in Section C above have been listed in the table below, and then grouped into five performance categories that would satisfy the requirements in various areas in a healthcare facility.
| WALL PROPERTIES | PERFORMANCE CATEGORY | |||
|---|---|---|---|---|
| 1 | 2 | 3 | 4 | |
| Smooth | ✓ | ✓ | O | O |
| Impervious | ✓ | ✓ | O | O |
| Jointless/seamless | ✓ | O | O | O |
| Textured | O | 🗴 | O | O |
| Perforated | O | 🗴 | O | O |
| Jointed | O | O | O | O |
| Low maintenance | ✓ | ✓ | ✓ | ✓ |
| Washable/easily cleaned | ✓ | ✓ | ✓ | O |
| Suited to high humidity areas | O | ✓ O |
🗴 ✓ |
🗴 |
| Acoustic priority | O | 🗴 | ✓ | 🗴 |
| Aesthetic priority | O | 🗴 | ✓ | 🗴 |
Legend/Key:
✓ – indicates this property is required for the class
🗴 – indicates this property is not required for the class
O – indicates this property is an optional requirement for the class
Examples of wall finishes for Class 1 (typical area – operating theatre):
- Enamel paint, epoxy coating, vinyl cladding or glazed partitions in special applications, etc.
Examples of wall finishes for Class 2 (typical area – dirty utility or ablution):
- Enamel paint, epoxy coating, porcelain or ceramic tiles, etc.
Examples of wall finishes for Class 3 (typical room – passage, restroom or waiting room):
- PVA paint, glazed partitions, wall-paper, timber panels or enamel paint, etc.
Examples of wall finishes for Class 4 (typical area – plant room):
- PVA paint, enamel paint, epoxy coating, etc.
Refer to Table 2 – Matrix of recommended wall performance categories to establish what performance category the wall of the room in question will require.
Performance categories recommended per room
| Department | Room Name | Wall Performance | ||||
|---|---|---|---|---|---|---|
| 1 | 2 | 3 | 4 | 5 | ||
| Acute Inpatient Wards (Adults) | Circulation Space | ⏺ | ||||
| Cleaners’ Room | ⏺ | |||||
| Consulting Room | ⏺ | |||||
| Day Lounge (patients) | ⏺ | |||||
| Dirty Utility Room (Sluice) | ⏺ | |||||
| Duty Room | ⏺ | |||||
| Equipment Store | ⏺ | |||||
| General Ward (single or multi-bed) | ⏺ | |||||
| Isolation Ward | ⏺ | |||||
| Kit Room | ⏺ | |||||
| Linen Room | ⏺ | |||||
| Office | ⏺ | |||||
| Patient Ablutions | ⏺ | |||||
| Patient-assisted Ablution | ⏺ | |||||
| Staff Ablutions | ⏺ | |||||
| Staff Change Room | ⏺ | |||||
| Staff Restroom | ⏺ | |||||
| Surgical Sundries Store | ⏺ | |||||
| Treatment Room | ⏺ | |||||
| Waiting Area (public) | ⏺ | |||||
| Ward Kitchen | ⏺ | |||||
| Ward Nurses’ Station | ⏺ | |||||
| Administration Department | Circulation | ⏺ | ||||
| Cleaners’ Room | ⏺ | |||||
| Offices/interview rooms | ⏺ | |||||
| Reception | ⏺ | |||||
| Boardroom | ⏺ | |||||
| Stores | ⏺ | |||||
| Kitchenette | ⏺ | |||||
| Records Room | ⏺ | |||||
| Print room | ⏺ | |||||
| Staff WCs | ⏺ | |||||
| Waiting Area (public) | ⏺ | |||||
| Casualty and Trauma | Circulation | ⏺ | ||||
| Cleaners’ Room | ⏺ | |||||
| Consulting Room | ⏺ | |||||
| Dirty Utility Room (Sluice) | ⏺ | |||||
| Duty Room | ⏺ | |||||
| Equipment Store | ⏺ | |||||
| Hazmat Shower | ⏺ | |||||
| Minor Theatre /Suture Room | ⏺ | |||||
| Observation Area | ⏺ | |||||
| Office | ⏺ | |||||
| Patient Ablutions | ⏺ | |||||
| Patient-assisted Ablution | ⏺ | |||||
| POPS Suite | ⏺ | |||||
| Public WCs | ⏺ | |||||
| Reception/Nurses’ Station | ⏺ | |||||
| Rehydration Area | ⏺ | |||||
| Resuscitation Area | ⏺ | |||||
| Scrub Area | ⏺ | |||||
| Staff Ablutions and Ablutions | ⏺ | |||||
| Staff Restroom | ⏺ | |||||
| Surgical Sundries Store | ⏺ | |||||
| Waiting Area (public) | ⏺ | |||||
| Central Sterilising and Supply Department (CSSD) | Dirty Utility | ⏺ | ||||
| Chemical Store | ⏺ | |||||
| Circulation | ⏺ | |||||
| Cleaners’ Room | ⏺ | |||||
| Dirty Linen | ⏺ | |||||
| Office | ⏺ | |||||
| Packing | ⏺ | |||||
| Plant Room | ⏺ | |||||
| Staff Change Room | ⏺ | |||||
| Staff Restroom | ⏺ | |||||
| Staff WCs | ⏺ | |||||
| Sterile Storage | ⏺ | |||||
| Sterilisation (autoclaves) | ⏺ | |||||
| Trolley Wash | ⏺ | |||||
| Washing and Disinfecting Area | ⏺ | |||||
| Community Health Centre | Circulation | ⏺ | ||||
| Cleaners’ Room | ⏺ | |||||
| Consulting Room | ⏺ | |||||
| Delivery Room | ⏺ | |||||
| Dental Surgery | ⏺ | |||||
| Dirty Utility Room (Sluice) | ⏺ | |||||
| Dispensary | ⏺ | |||||
| Duty Room | ⏺ | |||||
| Equipment Store | ⏺ | |||||
| Guard House or Security Kiosk | ⏺ | |||||
| Isolation/Separate Nursing Ward | ⏺ | |||||
| Linen Store | ⏺ | |||||
| Observation Area | ⏺ | |||||
| Office | ⏺ | |||||
| Offloading/Holding area for Pharmacy | ⏺ | |||||
| PABX /Server Rooms | ⏺ | |||||
| Patient Ablutions | ⏺ | |||||
| Patient-assisted Ablution | ⏺ | |||||
| Pharmacy | ⏺ | |||||
| Plant Room | ⏺ | |||||
| POPS Suite | ⏺ | |||||
| Public WCs and Change Rooms | ⏺ | |||||
| Reception/Nurses’ Station | ⏺ | |||||
| Records Room | ⏺ | |||||
| Recovery Area | ⏺ | |||||
| Rehydration Area | ⏺ | |||||
| Resuscitation Area | ⏺ | |||||
| Staff Ablutions | ⏺ | |||||
| Staff Change Room | ⏺ | |||||
| Staff Restroom | ⏺ | |||||
| Surgical Sundries Store | ⏺ | |||||
| Treatment Room | ⏺ | |||||
| Trolley Bay (entrances) | ⏺ | |||||
| Ultrasound Room | ⏺ | |||||
| Ward | ⏺ | |||||
| Waiting Area (public) | ⏺ | |||||
| X-Ray Room | ⏺ | |||||
| Day Clinic (Department) | Circulation Space | ⏺ | ||||
| Cleaners’ Room | ⏺ | |||||
| Consulting Room | ⏺ | |||||
| Dirty Utility Room (Sluice) | ⏺ | |||||
| Duty Room | ⏺ | |||||
| Equipment Store | ⏺ | |||||
| General Ward (single or multi-bed) | ⏺ | |||||
| Kit Room | ⏺ | |||||
| Linen Room | ⏺ | |||||
| Office | ⏺ | |||||
| Operating Theatre | ⏺ | |||||
| Patient Ablutions | ⏺ | |||||
| Patient Waiting | ⏺ | |||||
| Recovery Area | ⏺ | |||||
| Scrub Area | ⏺ | |||||
| Setting Area | ⏺ | |||||
| Staff Ablutions and Change Room | ⏺ | |||||
| Staff Restroom | ⏺ | |||||
| Surgical Sundries Store | ⏺ | |||||
| Treatment Room | ⏺ | |||||
| Waiting Area (public) | ⏺ | |||||
| Ward Kitchen | ⏺ | |||||
| Ward Nurses’ Station | ⏺ | |||||
| Dental Unit (Department) | Circulation Space | ⏺ | ||||
| Cleaners’ Room | ⏺ | |||||
| Consulting Room | ⏺ | |||||
| Dental Surgery | ⏺ | |||||
| Dirty Utility Room (Sluice) | ⏺ | |||||
| Equipment Store | ⏺ | |||||
| Panoral Room | ⏺ | |||||
| Patient Ablutions | ⏺ | |||||
| Reception /Office | ⏺ | |||||
| Records Room | ⏺ | |||||
| Staff Ablutions | ⏺ | |||||
| Staff Restroom | ⏺ | |||||
| Surgical Sundries Store | ⏺ | |||||
| Waiting Area (Public) | ⏺ | |||||
| High Care or Cardiac Care Unit
(HC/CCU) |
Circulation | ⏺ | ||||
| Cleaners’ Room | ⏺ | |||||
| Dirty Utility | ⏺ | |||||
| Duty Room | ⏺ | |||||
| Equipment Store | ⏺ | |||||
| Isolation Ward | ⏺ | |||||
| Linen Room | ⏺ | |||||
| Nurses’ Station | ⏺ | |||||
| Open Ward Area | ⏺ | |||||
| Patient Ablutions | ⏺ | |||||
| Staff Change Room | ⏺ | |||||
| Staff Restroom | ⏺ | |||||
| Staff WCs | ⏺ | |||||
| Surgical Sundries Store | ⏺ | |||||
| Ward Kitchen | ⏺ | |||||
| Intensive Care Unit (ICU) | Circulation | ⏺ | ||||
| Cleaners’ Room | ⏺ | |||||
| Dirty Utility | ⏺ | |||||
| Duty Room | ⏺ | |||||
| Equipment Store | ⏺ | |||||
| Isolation Ward | ⏺ | |||||
| Linen Room | ⏺ | |||||
| Nurses’ Station | ⏺ | |||||
| Open Ward Area | ⏺ | |||||
| Patient Ablutions | ⏺ | |||||
| Staff Change Room | ⏺ | |||||
| Staff Restroom | ⏺ | |||||
| Staff WCs | ⏺ | |||||
| Surgical Sundries Store | ⏺ | |||||
| Ward Kitchen | ⏺ | |||||
| Kitchen – (Main Hospital) | Bulk Dry Goods Store | ⏺ | ||||
| Chemical Store | ⏺ | |||||
| Cleaners’ Room | ⏺ | |||||
| Cold Room/Freezer | specialised | |||||
| Cooking Area | ⏺ | |||||
| Cutlery/Crockery Store | ⏺ | |||||
| Dishwashing and Potwashing Area | ⏺ | |||||
| Food Preparation Area | ⏺ | |||||
| Office | ⏺ | |||||
| Plating /Serving Area | ⏺ | |||||
| Receiving Area | ⏺ | |||||
| Staff Ablutions | ⏺ | |||||
| Staff Restroom | ⏺ | |||||
| Trolley Wash Area | ⏺ | |||||
| Laboratory (Pathology/Cytology/
Haematology/Chemistry) (Biosafety Level 2)
|
Blood and Blood Products Store | ⏺ | ||||
| Cell and Tissue Laboratory | ⏺ | |||||
| Cytopathology Sample Storage | ⏺ | |||||
| Clinical Material Store | ⏺ | |||||
| Disposal Area (dangerous materials) | ⏺ | |||||
| Drug and Vaccines Store | ⏺ | |||||
| Flammable Goods Store (external) | ⏺ | |||||
| Gas Cylinder and Pressure Vessel Store | ⏺ | |||||
| Hazardous Substances Store | ⏺ | |||||
| Histopathology Laboratory | ⏺ | |||||
| Microbiology Laboratory | ⏺ | |||||
| Offices | ⏺ | |||||
| POCT consulting room | ⏺ | |||||
| Reagents /Chemical Stores | ⏺ | |||||
| Records Rooms | ⏺ | |||||
| Sample Collection Laboratory | ⏺ | |||||
| Specimen Reception and Sorting rooms | ⏺ | |||||
| Stores (protective clothing/equipment) | ⏺ | |||||
| Staff Ablutions | ⏺ | |||||
| Staff Change Room including lockers | ⏺ | |||||
| Staff Restroom | ⏺ | |||||
| Laundry – (Main Hospital) | Assembly, Packing and Dispatch | ⏺ | ||||
| Chemical Store | ⏺ | |||||
| Circulation | ⏺ | |||||
| Cleaners’ Room | ⏺ | |||||
| Office | ⏺ | |||||
| Pressing | ⏺ | |||||
| Sorting | ⏺ | |||||
| Staff Ablutions | ⏺ | |||||
| Staff Restroom | ⏺ | |||||
| Stores | ⏺ | |||||
| Washing Room | ⏺ | |||||
| Maternity /Delivery Department | Baby Bathing Area | ⏺ | ||||
| Circulation | ⏺ | |||||
| Delivery Suite | ⏺ | |||||
| Dirty Utility Room | ⏺ | |||||
| Duty Room | ⏺ | |||||
| Equipment Store | ⏺ | |||||
| First Stage Room | ⏺ | |||||
| Kit Room | ⏺ | |||||
| Linen Store | ⏺ | |||||
| Milk Kitchen | ⏺ | |||||
| Nurses’ Station | ⏺ | |||||
| Nursery | ⏺ | |||||
| Patient Ablutions | ⏺ | |||||
| Staff Change Room | ⏺ | |||||
| Staff Restroom | ⏺ | |||||
| Staff WCs | ⏺ | |||||
| Surgical Sundries Store | ⏺ | |||||
| Viewing Area | ⏺ | |||||
| Waiting Area | ⏺ | |||||
| Ward Kitchen | ⏺ | |||||
| Wards | ⏺ | |||||
| Mental Health Facility | Body Room | ⏺ | ||||
| Children's Play Area | ⏺ | |||||
| Clean Utility | ⏺ | |||||
| Cleaners’ Room/Station | ⏺ | |||||
| Consulting Room | ⏺ | |||||
| Counselling Room | ⏺ | |||||
| Dirty Linen | ⏺ | |||||
| Dirty Utility (Sluice) | ⏺ | |||||
| ECT Procedure Room | ⏺ | |||||
| En Suite Bath/Shower Room | ⏺ | |||||
| Equipment Store | ⏺ | |||||
| Group Therapy Room | ⏺ | |||||
| Gymnasium (OT and Physio) | ⏺ | |||||
| IT Room | ⏺ | |||||
| Kit Room | ⏺ | |||||
| Linen Store | ⏺ | |||||
| Medicine Store | ⏺ | |||||
| Multi-Purpose Hall | ⏺ | |||||
| Nurses’ Station | ⏺ | |||||
| Office | ⏺ | |||||
| Patient-assisted Bathroom/Shower | ⏺ | |||||
| Patient Dining Room | ⏺ | |||||
| Patient Laundry | ⏺ | |||||
| Patient Lounge | ⏺ | |||||
| Pharmacy | ⏺ | |||||
| Quiet Room | ⏺ | |||||
| Records Room | ⏺ | |||||
| Seclusion Room | ⏺ | |||||
| Security Control Room | ⏺ | |||||
| Security Search Room | ⏺ | |||||
| Staff Change Room and WCs | ⏺ | |||||
| Surgical Sundries Store | ⏺ | |||||
| Treatment Room | ⏺ | |||||
| Wards | ⏺ | |||||
| Ward Kitchen | ⏺ | |||||
| Waste Disposal Room | ⏺ | |||||
| Mortuary | Blue Room | ⏺ | ||||
| Circulation Space | ⏺ | |||||
| Cleaners’ Room | ⏺ | |||||
| Dirty Utility | ⏺ | |||||
| Instruments Room | ⏺ | |||||
| Linen Room | ⏺ | |||||
| Medical Observation Room | ⏺ | |||||
| Office | ⏺ | |||||
| Pathologist Change Room | ⏺ | |||||
| Post-Mortem Room | ⏺ | |||||
| Staff Change Room | ⏺ | |||||
| Staff WCs | ⏺ | |||||
| Viewing Room | ⏺ | |||||
| Visitors’ Waiting Room | ⏺ | |||||
| Neonatal Intensive Care Unit (NNICU) | Circulation | ⏺ | ||||
| Cleaners’ Room | ⏺ | |||||
| Dirty Utility | ⏺ | |||||
| Duty Room | ⏺ | |||||
| Equipment Store | ⏺ | |||||
| Incubator Ward Area | ⏺ | |||||
| Isolation Ward | ⏺ | |||||
| Linen Room | ⏺ | |||||
| Milk Kitchen | ⏺ | |||||
| Mothers’ Rest Area | ⏺ | |||||
| Nurses’ Station | ⏺ | |||||
| Staff Change Room | ⏺ | |||||
| Staff Restroom | ⏺ | |||||
| Staff WCs | ⏺ | |||||
| Surgical Sundries Store | ⏺ | |||||
| Operating Theatre (Department) | Circulation | ⏺ | ||||
| Cleaners’ Room | ⏺ | |||||
| Dirty Utility | ⏺ | |||||
| Duty Room | ⏺ | |||||
| Equipment Store | ⏺ | |||||
| Nurses’ Station | ⏺ | |||||
| Operating Theatre | ⏺ | |||||
| Post-Operative Recovery Area | ⏺ | |||||
| Pre-Operative Holding Area | ⏺ | |||||
| Scrub-up Area/Room | ⏺ | |||||
| Setting Room | ⏺ | |||||
| Staff Change Room | ⏺ | |||||
| Staff Restroom | ⏺ | |||||
| Staff WCs | ⏺ | |||||
| Surgical Sundries Store | ⏺ | |||||
| Outpatients Department | Reception /Nurses’ Station | ⏺ | ||||
| Admissions Room | ⏺ | |||||
| Baby Changing Area | ⏺ | |||||
| Children’s Play /Waiting Area | ⏺ | |||||
| Circulation | ⏺ | |||||
| Consulting Room | ⏺ | |||||
| Dirty Utility Room | ⏺ | |||||
| Duty Room | ⏺ | |||||
| Equipment Store | ⏺ | |||||
| Kitchenette | ⏺ | |||||
| Linen Store | ⏺ | |||||
| Offices | ⏺ | |||||
| POPS Room | ⏺ | |||||
| Public Ablutions | ⏺ | |||||
| Records Room | ⏺ | |||||
| Staff Ablutions | ⏺ | |||||
| Staff Change Room | ⏺ | |||||
| Staff Restroom | ⏺ | |||||
| Surgical Sundries Store | ⏺ | |||||
| Treatment Room | ⏺ | |||||
| Waiting Areas (public) | ⏺ | |||||
| Wheelchair storage area | ⏺ | |||||
| Paediatric Ward | Child-assist Ablution | ⏺ | ||||
| Circulation Space | ⏺ | |||||
| Cleaners’ Room | ⏺ | |||||
| Consulting Room | ⏺ | |||||
| Dirty Utility (Isolation) | ⏺ | |||||
| Dirty Utility Room (Sluice) | ⏺ | |||||
| Duty Room | ⏺ | |||||
| Equipment Store | ⏺ | |||||
| General Ward (single or multi-bed) | ⏺ | |||||
| Isolation Ward | ⏺ | |||||
| Kit Room | ⏺ | |||||
| Linen Room | ⏺ | |||||
| Milk /Ward Kitchen | ⏺ | |||||
| Nurses’ Station | ⏺ | |||||
| Office | ⏺ | |||||
| Parent Ablutions | ⏺ | |||||
| Play Area (patients) | ⏺ | |||||
| Staff Change Room | ⏺ | |||||
| Staff Restroom | ⏺ | |||||
| Staff WCs | ⏺ | |||||
| Surgical Sundries Store | ⏺ | |||||
| Treatment Room | ⏺ | |||||
| Pharmacy/Dispensary | Cleaners’ Room | ⏺ | ||||
| Bulk Stores | ⏺ | |||||
| Circulation Space | ⏺ | |||||
| Counselling Cubicle | ⏺ | |||||
| Dispensary | ⏺ | |||||
| Liquid Filling Room | ⏺ | |||||
| Office | ⏺ | |||||
| Offloading Bay | ⏺ | |||||
| Patient Waiting Room | ⏺ | |||||
| Schedule Drugs Strong Room | ⏺ | |||||
| Staff Change Room | ⏺ | |||||
| Staff WCs | ⏺ | |||||
| Tablet Packing Room | ⏺ | |||||
| Vacolitre Stores | ⏺ | |||||
| Physiotherapy Department | Audiology Testing | ⏺ | ||||
| Circulation | ⏺ | |||||
| Consulting Room | ⏺ | |||||
| Equipment Store | ⏺ | |||||
| Gymnasium | ⏺ | |||||
| Kitchenette | ⏺ | |||||
| Occupational Therapy Room | ⏺ | |||||
| Patient Ablutions | ⏺ | |||||
| Reception | ⏺ | |||||
| Speech Therapy | ⏺ | |||||
| Staff Restroom | ⏺ | |||||
| Staff WCs | ⏺ | |||||
| Treatment Room | ⏺ | |||||
| Waiting Area | ⏺ | |||||
| Primary Health Clinic | Circulation | ⏺ | ||||
| Cleaners’ Room | ⏺ | |||||
| Consulting Room | ⏺ | |||||
| Delivery Room | ⏺ | |||||
| Dirty Utility Room (Sluice) | ⏺ | |||||
| Dispensary and Pharmacy | ⏺ | |||||
| Duty Room | ⏺ | |||||
| Equipment Store | ⏺ | |||||
| Guard House or Security Kiosk | ⏺ | |||||
| Linen Store | ⏺ | |||||
| Observation /Rehydration Area | ⏺ | |||||
| Office | ⏺ | |||||
| Public Ablutions | ⏺ | |||||
| Plant Room | ⏺ | |||||
| POPS Suite | ⏺ | |||||
| Reception/Nurses’ Station | ⏺ | |||||
| Records Room | ⏺ | |||||
| Staff Ablutions and Change Room | ⏺ | |||||
| Staff Restroom | ⏺ | |||||
| Surgical Sundries Store | ⏺ | |||||
| Treatment Room | ⏺ | |||||
| Trolley Bay (entrances) | ⏺ | |||||
| Waiting Area (public) | ⏺ | |||||
| Radiology (Diagnostic) | Bucky Room (general X-ray Room) | ⏺ | ||||
| Change Cubicles | ⏺ | |||||
| Circulation | ⏺ | |||||
| Cleaners’ Room | ⏺ | |||||
| CT /MRI Scan Room | ⏺ | |||||
| Dirty Utility /Sluice | ⏺ | |||||
| Fluoroscopy Room | ⏺ | |||||
| Fluoroscopy Control Room | ⏺ | |||||
| Inpatient Waiting Area | ⏺ | |||||
| Kitchenette | ⏺ | |||||
| Linen Room | ⏺ | |||||
| Mammogram Room | ⏺ | |||||
| Office | ⏺ | |||||
| Patient Ablutions | ⏺ | |||||
| Public Waiting Area | ⏺ | |||||
| Porters and Wheelchair/Trolley Parking | ⏺ | |||||
| Reception | ⏺ | |||||
| Records Room | ⏺ | |||||
| Server Room | ⏺ | |||||
| Staff Restroom | ⏺ | |||||
| Staff WCs | ⏺ | |||||
| Stores (Equipment/General) | ⏺ | |||||
| Ultrasound Room | ⏺ | |||||
| Telemedicine Room | ⏺ | |||||
| Viewing Room/CR Room/Reporting Area | ⏺ | |||||
| Nurses’ Residences | Ablutions | ⏺ | ||||
| Bedrooms | ⏺ | |||||
| Circulation | ⏺ | |||||
| Kitchenette | ⏺ | |||||
| Lounge | ⏺ | |||||
| Offices | ⏺ | |||||
| Public Ablutions | ⏺ | |||||
| Reception | ⏺ | |||||
| Stores | ⏺ | |||||
| Waiting Areas (public) | ⏺ | |||||
DEFINITIONS
Terminology
| Aggregation | Collected together from different sources and considered a whole. |
|---|---|
| Ambulant/ambulatory | (of a patient) Being able to walk or move around; not being confined to a bed. |
| Bacteriostatic | A word used to describe the property of a material that claims to inhibit the multiplication of bacteria. |
| Bariatric | Describing the condition of obesity. |
| Bonded | Chemically attached or fused in layers. |
| Emulsion | In the context of paint – referring to water-based paint that is not shiny when dry. |
| Guarantee | A document setting out a promise of quality made by a manufacturer or the provider of a service, a formal promise that a product will be repaired free of charge if it breaks or fails within a particular period or that substandard work will be redone. |
| Homogenous | Consisting of things of similar type throughout. |
| Heterogeneous | Consisting of various layers or types throughout. |
| Hygroscopic | Readily absorbing moisture from the atmosphere. |
| Hydrophobic | Water-repellent. |
| Impervious | Not allowing passage through (usually of water/moisture). |
| Interstices | Small holes or perforations. |
| Jointed | Junctions which may be open or covered, but not completely sealed and smooth. |
| Jointless | Without joints or having joints that are sealed by materials and methods that make the whole surface imperious and prevent the collection of dirt and bacteria in the joint. |
| Olfactory | Relating to the smell or the sense of smell. |
| Perfusion | Inject liquid into tissue or organ by circulating through blood vessels in the body. |
| Polyamide | Aa synthetic polymer made by the linkage of an amino group of one molecule and a carboxylic acid group of another, including many synthetic fibres such as nylon. |
| Resilient finish | The quality of a material to spring back quickly into shape after being bent, stretched or squashed. |
| Seamless | A surface without open joints or junctions, or where such joints are completely sealed and smoothed to create a continuous and whole membrane. |
| Smooth surface | A flat surface without projections, indentations or perforations such as a brush-painted plastered surface. |
| Textured | A surface finish that is not smooth, but has a fissured/embossed or ridged finish. |
| Vitrified | To change a material into glass, under high heat and other conditions. |
| Washable | A term implying that a finish can be repeatedly and regularly cleaned using water and water-diluted cleaners without detrimental effect to the finish. |
| Warranty | A written promise to repair or replace a product that has a manufacturing fault. This commonly comes with conditions and is limited to a time-frame given at the time of purchase. |
Abbreviations
| BRE | Building Research Establishment |
|---|---|
| CHD | Center for Health Design |
| ENT | Ear, Nose and Throat |
| HAI | Healthcare-associated infections |
| HDF | High-density fibreboard |
| IAQ | Indoor Environmental Quality |
| IEQ | Indoor Environmental Quality |
| IUSS | Infrastructure Unit Systems Support |
| MDF | Medium-density fibreboard |
| MRSA | Methicillin-resistant Staphylococcus Aureus, which is a common skin bacterium that is resistant to a range of antibiotics otherwise referred to as multi-drug resistant bacteria |
| NDoH | National Department of Health |
| OoM | Order of Magnitude |
| PMIS | Project Management Information System |
| PMSU | Project Management Support Unit |
| PUR | Polyurethane-resistant |
| PVC | Polyvinyl-chloride |
| RC | Recommendation Committee |
| SANS | South African National Standard |
| TIG | Tungsten inert gas |
| VOC | Volatile organic compound |
| VRE | Vancomycin-resistant Enterococci (drug-resistant bacteria that can lead to HAIs) |
REFERENCES
Bibliography
Alcorn, A. and Wood, P., 1998. New Zealand building materials embodied energy coefficients database. (Volume II-Coefficients). Wellington, New Zealand: Centre for Building Performance Research.
Cement & Concrete Institute (CCI), 2009. Sand-cement screeds and concrete toppings for floors. [pdf] Midrand, South Africa: CCI. Available at: http://www.afrisam.co.za/media/13770/Sand_cement_floor_screeds_and_concrete_toppings_for_floors.pdf[Accessed 9 April 2014].
Center for Health Assets Australasia, 2009. Floor coverings in healthcare buildings. (Technical series TS-7 version 1.1). New South Wales:NSW Health.
Dean, Y., 1996. Finishes. 4th ed. Harlow, UK: Addison Wesley Longman Ltd.
Department of Health (DH), 2010. Core elements: Health Building Note 00-03: Clinical and clinical support spaces. UK: DH.
Department of Health (DoH), 1980. Regulations governing private hospitals and unattached operating theatres. (Government notice No. R.158 of the Health Act, 1971. (C.63). Cape Town South Africa: Government Gazette.
Department of Health Finance and Investment Directorate Estates and Facilities Division, 2006. Health Technical Memorandum 61: Building component series flooring. [pdf] London: The Stationery Office. Available at: http://www.wales.nhs.uk/sites3/Documents/254/HTM%2061%202006.pdf [Accessed 9 April 2014].
Department of Health Gateway Review, Estates & Facilities Division, 2011. Performance requirements for building elements used in healthcare facilities. (Version:0.6:England). [pdf] Leeds: HMSO. Available at: http://www.derbyshirelmc.org.uk/Guidance/8941-England-8941_0.6_England.pdf [Accessed 9 April 2014].
Department of Health, n.d. R&D project B(04)02: Developing an integrated system for the optimal selection of hospital finishes. Aberdeen, Scotland: Department of Health.
HermanMiller Healthcare, 2006. Sound practices: Noise control in the healthcare environment. (Research summary/2006). Zeeland, Michigan: Herman Miller.
Joseph, A., 2006. The impact of light on outcomes in healthcare settings. Concord, CA: The Center for Health Design. Available at: http://www.healthdesign.org/sites/default/files/CHD_Issue_Paper2.pdf [Accessed 9 April 2014].
Joseph, A., Malone, E., Pati, D. and Quan, X., 2011. Healthcare environmental terms and outcome measures: An evidence-based design glossary. Concord, CA:The Center for Health Design.
Jung, W.K., Koo, H.C., Kim, K.W., Shin, S., Kim, S.H. and Park, Y.H., 2008. Antibacterial activity and mechanism of action of the silver ion in staphylococcus aureus and escherichia coli. Applied and Environmental Microbiology, 74(7), pp.2171-2178.
Lavy, S., 2010. Facility managers’ preferred interior wall finishes in acute-care hospital buildings. In: CIB, 18th CIB World Building Congress: Facilities management and maintenance. Salford, United Kingdom, 10-13 May 2010. Salford, United Kingdom: CIB.
Makison, C. and Swan, J., 2005. The effect of humidity on the survival of MRSA on hard surfaces. (R&D report B(03)02). [pdf] London: Estates and Facilities Division of the Department of Health. Available at: http://www.wales.nhs.uk/sites3/Documents/254/B(03)02%20MRSA.pdf [Accessed 9 April 2014].
Nanda, U., Malone, E. and Joseph, A., 2012. Achieving EBD goals through flooring selection & design. [pdf] Concord, CA:The Center for Health Design. Available at: http://www.healthdesign.org/sites/default/files/chd_achieving_ebd_goals_through_flooring__design_final_0.pdf [Accessed 9 April 2014].
NHS Estates, 2005. Health Technical Memorandum (HTM) 56: Building component series: Partitions. UK: TSO.
NHS Estates, 2005. Health Technical Memorandum (HTM) 60: Ceilings. 2nd ed. UK: TSO.
NHS, National Services Scotland, 2006. Scottish Health Technical Memorandum (SHTM) 61: Building component series: Flooring. Scotland:Health Facilities Scotland.
NHS, National Services Scotland, 2007. Scottish Health Facilities Note 30: Infection control in the built environment: Design and planning. (Version 3). Scotland:Health Facilities Scotland.
NHS, National Services Scotland, 2009. Scottish Health Technical Memorandum (SHTM) 61: Building component series: Flooring. Scotland:Health Facilities Scotland.
PricewaterhouseCoopers LLP (PwC) in association with the University of Sheffield and Queen Margaret University College, 2004. The role of hospital design in the recruitment, retention and performance of NHS nurses in England. (Full report). [pdf] Edinburgh: Commission for Architecture and the Built Environment (CABE). Available at: http://webarchive.nationalarchives.gov.uk/20110118095356/http:/www.cabe.org.uk/files/the-role-of-hospital-design.pdf [Accessed 9 April 2014].
Tofle, R.B., Schwartz, B., Yoon, S., Max-Royale, A., 2003. Color in healthcare environments: A critical review of the research literature. California: The Coalition for Health Environments Research (CHER).
Ulrich, R. S. P., Zimring, C. P., Zhu, X., Dubose, M., Seo, H. B., Choi, Y. S. and Joseph, A. P., 2008. A review of the research literature on evidence-based healthcare design (Part II). Health Environments Research & Design Journal, 1(2008), 61-125.
Welsh Health Estates, 2009. Health Building Note 04-01: Adult in-patient accommodation. Cardiff, Wales:Welsh Health Estates.
Websites: Further reading
'''Error! Hyperlink reference not valid.'''(Health Technical Manuals – United Kingdom)
'''Error! Hyperlink reference not valid.'''(Precautionary Lists of Building Ingredients related to health effects and risks)
'''Error! Hyperlink reference not valid.'''(Sustainable Flooring benefits Hospitals in a variety of ways)
http://www.GreenhealthMagazine.org
http://greenhomeguide.com (Are Engineered wood products from Decorative Flooring a low VOC product? Joel Hirschberg, 2011)
http://gbcsa.org.za (IEQ rating tools)
http://www.green-buildings.com (Green Flooring: Linoleum, Marmoleum and Vinyl – Claire Maloney, LEED Green Associate, Cornell University 2013)
http://www.healthcaredesignmagazine.com (Five need to know trends shaping healthcare Design – K. Edmundson, 2011)
http://www.carpet-rug.org/documents/technical-bulletins (Carpet Treatments)
http://www.floorworx.co.za (Vinyl wall cladding and protection manufacturer)
http://www.polyflor.co.za (Vinyl wall cladding and protection manufacturer)
http://www.sassda.co.za (South African Stainless Steel Development Association)
PHOTOGRAPHIC AND ILLUSTRATION CREDITS
| Cover photo: | R. van Rensburg |
|---|---|
| Fig.1-2 | M. Swinney |
| Fig.3 | G. Abbott- CSIR |
| Fig.4 | R. Cubbin based on Life Cycle Floor Cost Table – by Nora®, USA |
| Fig.5 | R. Cubbin |
| Fig.6-7 | M. Swinney |
| Fig.8 | R. van Rensburg |
| Fig.9-14 | M. Swinney |
| Fig.15 | R. van Rensburg |
| Fig.16 | R. van Rensburg |
| Fig.17 | R. van Rensburg |
| Fig.18-24 | M. Swinney |
| Fig.25 | R. van Rensburg |
| Fig.26-27 | M. Swinney |
| Fig.28 | C. Hudson |
| Fig.29 | R. van Rensburg |
| Fig.30 | M. Swinney |
| Fig.31 | R. van Rensburg |
| Fig.32-34 | M. Swinney |
| Fig.35 | R. Cubbin |
| Fig.36-38 | M. Swinney |
| Fig.39-40 | R. van Rensburg |
| Fig.41 | M. Swinney |
| Fig.42-44 | R. van Rensburg |
| Fig.43 | M. Swinney |
| Fig. 44 | R. Cubbin |
| Fig.45 | M. Swinney |